|
1) Introduction/consent/indications/wash hands/name & age of patient/asks patient for sites of pain before commencing
2) General Inspection
- Student inspects all around the ear, and assess for any skin pits or tags
- Inspect pinna and assess deformities
- Look behind ear for surgical scars (mastoidectomy)
- Press tragus, pain indicates external auditory canal infection
- Pull pinna for pain, and gently press mastoid process – positive in mastoiditis
- Repeat procedure on opposite ear
3) Auroscope examination:
- Student explains procedure, asks if patient has any questions, and to notify if any pain occurs
- Pulls pinna superior and posteriorly to straighten external auditory meatus
- Auroscope is held like a pen, and in the same hand as the ear examined
- Examines the external canal commenting on any flaking (eczema), a swollen, narrow canal with foul smelling discharge (otitis externa), wax and any evidence of a foreign body
- Examines the tympanic membrane, commenting on:
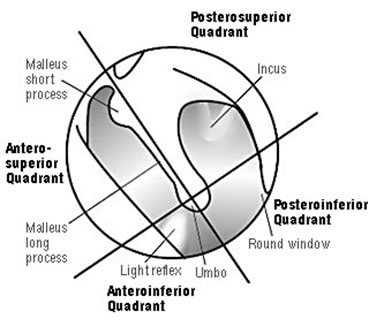
1. Light reflex/ cone of light
2. Colour: Should be pearly/ pinky grey
3. Tympanosclerosis: Previous trauma & subsequent scarring
4. Fluid level indicates: Otitis media, with persistent otitis media leading to thickened fluid and thus glue ear – treated by grommets
5. Indrawing of the tympanic membrane and prominent short process of the malleus indicates eustachian tube dysfunction. Asks patient to perform valsalva, which in normal individuals leads to protrusion of ear drum
6. Any perforations: Usually subtotal, with a 60dB hearing loss
4) Perform Weber’s & Rinne’s Tests:
- Student commences exam by whispering a word in first ear (30cm distance), whilst masking contralateral ear by rubbing the tragus. Student asks patient to repeat whispered words, and then proceeds to repeat process in the contralateral ear
- Before commencing Weber’s or Rinne’s tests, student correctly identifies that a 512Hz tuning fork is to be utilised. To vibrate tuning fork, tap on knee or elbow, and NOT on a wooden or metallic object
- Weber’s test performed first: Asks patient to confirm whether sound is central (normal) or lateralises to one ear. Sound lateralises to specific ear if there is a conductive hearing loss in that ear or sensorineural hearing loss in the opposite ear
- Rinne’s test: If sound lateralises to one ear on Weber’s test, student commences Rinne’s on same ear. Applies tuning fork to mastoid process and asks patient when sound disappears. When sound disappears, student places the tuning fork in front of the ear and asks if they can hear sound.
- Test results:
1. Weber’s lateralises to left, and Rinne’s –ve (BC>AC) = conductive hearing loss in left
2. Weber’s lateralises to left, and Rinne’s +ve (AC>BC), testing opposite ear, demonstrates
Rinne’s +ve = sensorineural hearing loss in right
5) Vestibular Function:
- Assessed by a Dix-Hallpike’s test, and generally positive in benign paroxysmal positional vertigo, as well as vestibular neuronitis, Meniere’s disease and cerebral masses:
1. Commenced with patient sitting upright & legs extended
2. Head is rotated by 45 degrees
3. Patient is then put into a supine position quickly with the head held slightly extended below
couch level (~20 degrees)
4. Patient's eyes are observed for 45 secs, due to a 5-10 second latency period prior to nystagmus. Rotational nystagmus is considered +ve for BPPV (fast phase of rotatory nystagmus is towards
affected ear / that closest to the ground)
- Examination ended by stating that they would examine for any lymph nodes, and perform pure tone audiometry
6) Thanks patient & documents findings in the notes:
Author:
Mr Adnan Darr MBCHB, BSc, MSc, MRCS
| Speciality:
Examination
| Date Added:
02/11/2011
|