|
TAP blocks are relatively easy and quick to perform with few associated risks. It can provide good analgesia for up to 48h postoperatively, resulting in decreased opioid requirements and facilitating earlier mobilisation. Note that TAP blocks only provide analgesia of the abdominal wall and no visceral analgesia, so some opiate administration perioperatively is still required.
Indications
Unilateral TAP block: for appendicectomy, inguinal hernia repair, femoral hernia repair, cholecystectomy
Bilateral TAP block: for midline laparotomy, laparoscopic abdominal/pelvic surgery, C-section, total abdominal hysterectomy
Anatomy
Source: AAGBI
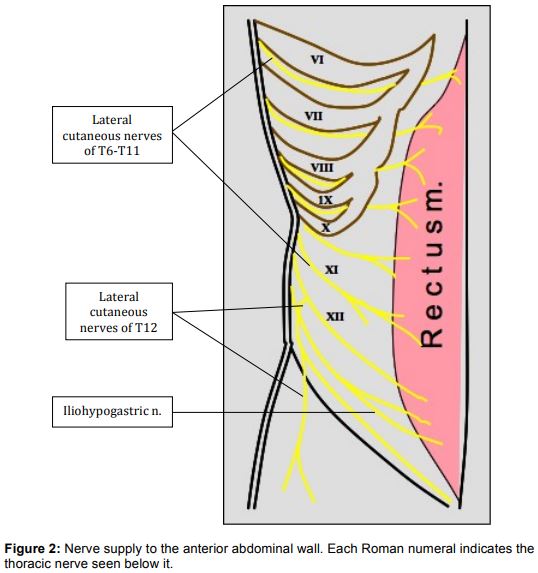
The anterior abdominal wall is innervated by thoracolumbar segmental nerves T6-L1. These nerves travel in the neurofascial (TAP) plane between internal oblique and transversus abdominis, until the mid-axillary line when a cutaneous branch pierces the internal and external oblique muscles to supply the skin of the anterior abdominal wall. The rest of the nerve continues down to pierce the posterior rectus sheath to supply the skin midline of abdomen.
Source: AAGBI
The lumbar triangle of Petit is where the external and internal oblique muscles become fascia prior to insertion into perilumbar fascia. This landmark is found posterior to the midaxillary line, bounded posteriorly by the lateral edge of latissimus dorsi, anteriorly by external oblique muscle, inferiorly by iliac crest and with external oblique aponeurosis as the floor.
Complications: Vascular injection, peritoneal perforation
Technique
- Position patient supine
Tip: the operator should stand contralateral to the block side for best control of needle. In the obese patient, the adipose layer is usually attenuated at the level of the iliac crest and displacement of surplus skin and adipose tissue cranially by an assistant will aid performance of block.
- Identify the lumbar triangle of Petit by palpating the lateral border of latissimus muscle just superior to the iliac crest and posterior border of the external oblique muscle.
Tip: Lateral displacement of the lower limbs away from the side of block aids identification of the lumbar triangle of Petit by stretching the fascial layers.
- Insert needle about 1cm cranial to iliac crest
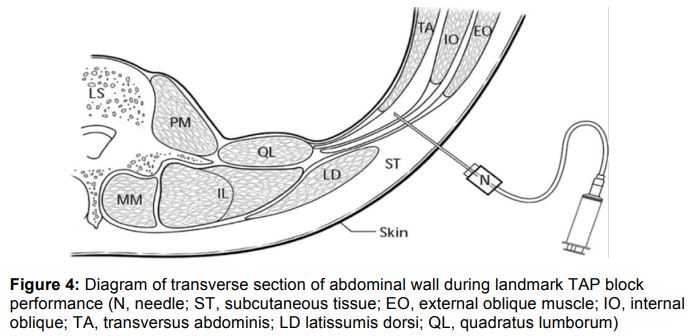
- Gentle advancement of the needle results in a 'pop' sensation as the needle pierces the external oblique fascia. Further gentle advancement results in a second 'pop' as the needle pierces the internal oblique fascia and enters the transversus abdominus fascial plane.
- Aspirate to exclude vascular puncture then administer 20-30ml LA
References
Warman P, Conn D, Nicholls B, Wilkinson D. Regional Anaesthesia, Stimulation, and Ultrasound Techniques. Oxford Specialist Handbooks in Anaesthesia.
Author:
Ms Yanyu Tan
| Speciality:
Anaesthetics/ICU
| Date Added:
09/11/2018
|